Introduction
The life expectancy of the Indian population is on a rise, leading to steadily increasing number of complex resorbed complete denture patients every year. Practical objectives of complete denture therapy for patients with such ridges include the placement of functional and esthetic dentition substitutes and the replacement of associated dental supporting structures. In so doing, the prostheses often occupy a substantial volume within the edentulous oral cavity. In addition to simply replacing missing oral tissues, complete dentures serve to structurally redefine true spaces and potential spaces within the oral cavity.[1] Regardless of the fabrication technique used, functionally inappropriate denture tooth arrangement or physiologically unacceptable denture base volume or contour have been implicated in poor prosthesis stability and retention, compromised phonetics, inadequate facial tissue support, inefficient tongue posture and function and hyperactive gagging.
The statistics show that patients with severe resorption are opting for either implants or get new dentures made every year. Dental implants may provide stabilization of mandibular complete dentures for the atrophic mandible, however there may be situations when it is not possible to provide implants on the grounds of medical, surgical or costs factors. Therefore, the neutral zone technique is an alternative approach for such cases. The technique is not new but is one that is valuable and yet not often practiced.[2]
The neutral zone has been defined as the area/ zone in the mouth where during function, the forces of the tongue pressing outwards are neutralised by the forces of the cheeks and lips pressing inwards. This zone is also referred to as “zone of minimal conflict”, “dead space”, “denture space”.[3]
The two men who probably have contributed the most to these concepts are Wilford Fish and Russell Tench.
• Sir Wilfred Fish first described the influence of the polished surfaces on retention and stability in 1931. He also described how dentures should be constructed in the 'dead space', which later became known as the neutral zone.
• Fish had stated “The fundamental principle in the construction of full dentures is that every part of every surface of the denture shall be modeled to fit some part of the patient’s tissues, or some part of the other denture.” [4]
This technique has been referred to in the past as the “anthropoidal pouch technique”, “muscle formed mandibular denture technique”, or “denture form impression technique.
This denture space is bounded by the maxilla and soft palate above, by the mandible and floor of the mouth below, by the tongue, medially or internally, and by the muscles and tissues of the lips and cheeks laterally or externally[5].
Heath (1970) has demonstrated that there is a difference in the shape of the denture space and resultant arch form at rest as compared to the denture space and arch form established by function[6].
The lower denture commonly presents the most difficulties with pain and looseness being the most common complaint.[7] This is because the mandible atrophies at a greater rate than the maxilla and has less residual ridge for retention and support.[8] The neutral zone technique is most effective for patients who have had numerous unstable, unretentive lower complete dentures. These patients usually have a highly atrophic mandible and there has been difficulty in positioning the teeth to produce a stable denture.
The neutral zone approach has also been used for patients who have had: a partial glossectomy, mandibular resections or motor nerve damage to the tongue disease, trauma or burns, a stroke, scleroderma, or conditions arising from other natural causes such as prominent mental groove.[9]
A denture shaped by the neutral zone will have advantages:
• Improved stability and retention
• Posterior teeth will be correctly positioned allowing sufficient tongue space
• Reduced food trapping adjacent to the molar teeth
• Good aesthetics due to facial support.[2]
The aim of this article is to describe the neutral zone technique in patients with severely resorbed edentulous ridge.
Case Report
A 60 year old female patient came to the Department of Prosthodontics and Crown and Bridge with chief complaint of loose and unstable lower denture and wanted the replacement for the same. On intraoral examination it was found that the patient was completely edentulous with resorbed of both the arches [Figure: 1, 2].
 | Fig.1 - Pretreatment Extraoral View
 |
 | Fig.2 - Pretreatment Intraoral View
|
Patient also gave a history of dissatisfaction with the previous set of denture fabricated 9 months back. A treatment plan was made which included fabrication of upper and lower removable complete dentures with incorporation of neutral zone concept for construction of mandibular denture. The patient was explained the same.
Primary impression of the maxillary and mandibular edentulous residual ridge was made with modelling plastic compound impression material. The impression was poured in plaster of paris and primary casts were prepared.
The custom trays were fabricated with self cure resin over the primary casts keeping the borders 2mm short of the sulcus. The borders of the trays were moulded with green stick impression compound and the secondary impressions were made with zinc oxide eugenol impression material. The master casts were poured in dental stone plaster.
Record bases were prepared in self cure resin on master casts. Wax occlusal rims were made over the temporary record bases for recording the jaw relations. The vertical dimension and centric relation was obtained in the usual manner. Warm 2 parts of red and 1 stick of green modeling plastic impression compound (Impression Compound; Kerr Corp), knead the material thoroughly, and adapt it to the record base, forming a superstructure for the tissue conditioner and place it over the mandibular record base. It is sealed properly with a heated spatula.
A high viscous mix of tissue conditioner (Viscogel Dentsply, Weybridge, UK) is advocated for the impression. The mix is placed along the base plate and superstructure. The volume of the material should be controlled and kept to a minimum so that the sulci are not distorted. The material is mixed so that it can be manipulated by hand and positioned as an approximate rim on the lower base plate. The maxillary record base is not used to avoid the compressive interferences if occlusal contacts are encountered during this functional recording procedure.
The patient is asked to sit in a comfortable, upright position with the head supported. The occlusal rim is then placed inside the patient’s mouth and is asked to perform a series of actions designed to simulate physiological functioning. These actions include include asking the patient to: smile, grin, pout/purse lips, count from 60 to 70, pronounce the vowels, sip water, swallow, slightly protrude the tongue and lick the lips. These actions were repeated for 10 minutes until material has set. The neutral zone impression is then seated on the mandibular definitive cast [Figure: 3].
 | Fig.3 - Tissue Conditioner Used To Record Neutral Zone
|
Prepare laboratory putty (Poly V Putty; Accurate Set, Inc, Newark, NJ) to a workable consistency and adapt it into the tongue space and along the facial contours of the neutral zone record. (Fig 3). Mold the putty so that it: (a) completely fills the tongue space and captures accurately the facial contours, (b) is level with the occlusal plane of the record; and (d) extends over the posterior land area of the cast. After complete polymerization of the putty, the individual indices are removed such that they can be accurately placed back into the same position without the record [Figure: 4].
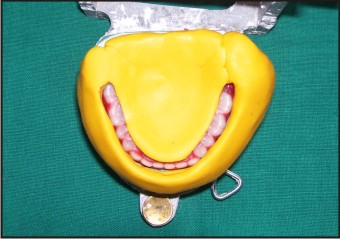 | Fig.4 - Silicone Putty Index Made
|
Maxillary anterior teeth are placed first. A new mandibular record base is made and teeth arrangement is done using the indices. After complete try- in, wax up is done with slight contouring of the borders so that they stay in the neutral zone. Dentures are processed in the conventional way. The dentures were finished and polished, and inserted in the patient's mouth [Figure: 5, 6].
 | Fig.5 - Finished And Polished Dentures
|
 | Fig.6 - Post Insertion Intraoral View
|
Patient was called after 24 hours, 1 week and 1 month for the follow dentures. Patient was satisfied with the new denture and reported increased retention and stability of the mandibular denture [Figure: 7].
 | Fig.7 - Post Insertion Extraoral View
|
Discussion
The neutral zone approach to complete denture construction is neither new nor original but, rather, constitutes the bringing together of the concepts and ideas of many men into a viable and practical procedure. This philosophy is based upon the concept that for each individual patient there exists within the denture space a specific area where the function of the musculature will not unseat the denture and where forces generated by the tongue are neutralized by the forces generated by the lips and cheeks.
As the period of edentulousness increases, the mandibular ridge resorbs from the lingual side in the molar region. By this pattern of resorption the arch will become wider in the posterior region. So the position of the neutral zone is lingual to crest of the alveolar ridge. So mandibular posterior teeth should be placed towards the lingual side and the discrepancy in this position increases as time apses, this is in accordance to Martone’s (1963) conclusions.The influence of tooth position and flange contour on denture stability is equal to or greater than that of any other factor. The technique is relatively simple but there are increased chair time and laboratory cost.
The neutral zone approach registers the zone of minimum conflict to determine the proper placement of teeth after resorption has taken place. In the absence of neutral zone principle the location of teeth are purely arbitrary. The awareness of neutral zone has been given importance due to increased risk of instability of the lower denture. The standard approach of placing the artificial teeth on the crest of the ridge is not in any means true to the original location of natural teeth. In other words, we should not be dogmatic in insisting that teeth should always be placed over the crest of the ridge or lingual to the crest of the ridge to obtain favourable teeth to ridge relation. The placement of teeth should be dictated by the lingual and buccal musculature, which will vary from patient to patients.
Conclusion
A thorough understanding of the anatomy and physiology of structures that impact sound complete denture fabrication and function is important for successful treatment of edentulous patients. Use of the neutral zone method to the identify and register the anatomy and physiology that impact prosthesis stability may result in improved prosthodontic therapy for patients.
References
1. David R. Cagna: The neutral zone revisited: From historical concepts to modern application J Prosthet Dent 2009;101:405-412
2. M. J. Gahan and A. D. Walmsley: The neutral zone impression revisited. BRITISH DENTAL JOURNAL VOLUME 198 NO. 5 MARCH 12 2005.
3. Beresin V E, Schiesser F J. The neutral zone in complete and partial dentures p 15. C.V. Mosby Co., 1978
4. Fish E W. An analysis of the stabilising factors in full denture construction. Br Dent J 1931; 52: 559–570.
5. Fish E W. Using the muscles to stabilize the full lower denture. J Am Dent Assoc 1933; 20: 2163–2169
6. Heath R. A study of the morphology of the denture space. Dent Practit 1970; 21: 109–117.
7. Basker R M, Harrison A, Ralph J P. A survey of patients referred to restorative dentistry clinics. Br Dent J 1988; 164: 105–108
8. Atwood D A. Post extraction changes in the adult mandible as illustrated by micrographs of midsagitall sections and serial cephalometric roentgenograms. J Prosthet Dent 1963; 13: 810–824.
9. Ohkubo C, Hanatani S, Hosoi T, Mizuno Y. Neutral zone approach for denture fabrication for a partial glossectomy patient: A clinical report. J Prosthet Dent 2000; 84: 390–393.
|